As I write to you, it’s evident that Covid-19 (C-19) cases and hospitalizations are increasing in many countries and new variants keep emerging.
The KP.3 variant is now spreading at a rapid rate and expected to soon dominate the evolutionary landscape of this immune escape pandemic. Given the uptick in disease and hospitalization cases, it becomes increasingly difficult for health authorities to hide their concern about the evolutionary dynamics of SARS-CoV-2 (SC-2). Despite this, they are trying to reassure the broader public (and especially themselves!) with the empty encouragement to get vaccinated again as soon as possible with the ‘spring vaccine’.
“However, do not expect much COVID-19 News coverages about the rise of the KP.3 variant or about its possible capability to contribute to increased disease severity and rise in hospitalizations and mortality as most governments are either trying to downplay or conceal the actual COVID-19 crisis as they wish to pursue their narratives that the COVID-19 vaccines provided protection against all who had them in the past or that it will still protect against the new variants!”
https://www.thailandmedical.news/news/forget-about-sars-cov-2-flirt-variants-kp-1-1-and-kp-2-new-fluqe-variant-kp-3-expected-to-rapidly-become-globally-predominant-wreaking-havoc#google_vignette
But what about the advice of experts and scientists?
Based on in vitro assays of sera from vaccinated animals or individuals previously infected, or vaccinated, some influential scientists are concluding that JN.1 exposure/ immunization induces a higher virus-neutralizing effect towards newly emerging variants (e.g., FLiRT mutants [JN.1+346T+456L] and KP.3) compared to XBB, which serves as the basis for the updated C-19 vaccines (https://www.biorxiv.org/content/10.1101/2024.04.19.590276v1.full.pdf).
However, these scientists seem to overlook or ignore that the term ‘neutralization’ they are using isn’t indicative of a genuine virus-neutralizing effect as the antibodies (Abs) they measure do not specifically bind to ACE2-competitive binding sites on the spike (S) protein). Their alleged neutralizing effect stems from their low affinity for S protein, which leads them to primarily engage in multivalent, avidity-based binding to the virus. Consequently, the infection-inhibitory effect of these low-affinity anti-S(pike) Abs diminishes rapidly, resulting in short-lived immunity. This situation is now leading to the exposure of large portions of highly C-19 vaccinated populations to suboptimal immunity. Suboptimal immune responses in large parts of the population inevitably cause highly C-19 vaccinated populations to collectively exert immune selection pressure on viral infectiousness, and eventually on viral transmissibility. I’ve repeatedly explained how this evolution will ultimately lead to the emergence of a new viral lineage with enhanced virulence in highly C-19 vaccinated populations.
As these scientists appear to lack a fundamental understanding of evolutionary biology, their interpretations lead their peers, as well as public health authorities, to believe that the generated data suggest that future C-19 vaccine efforts should “focus on the JN.1 lineage instead of XBB to better counter current and emerging variants”! (https://www.biorxiv.org/content/10.1101/2024.04.19.590276v1.full.pdf).
Another dramatic misconception about the current epidemiological situation is that, contrary to what some immunologically incompetent ‘experts’ suggest, this virus is not “on the way to becoming seasonal and becoming just another cause of the common cold” (https://www.dailymail.co.uk/health/article-13416469/Health-chiefs-issue-alert-new-Covid-variant-FLiRT-sweeping-UK.html). These self-proclaimed experts are asserting that “a wall of immunity built up among the population following repeated waves of infection and vaccine rollouts”! These guys do not realize that this ‘wall of immunity’, commonly known as ‘herd immunity,’ does not develop in highly C-19 vaccinated populations due to viral immune escape!
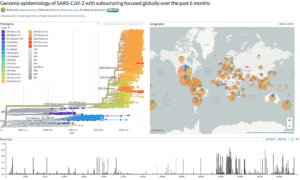
The low levels of productive infection (reflected by rather low virus concentrations in wastewater), together with the low incidence of acute C-19 disease they’re often referring to, constitute a kind of ‘fake’ (‘pseudo’) herd immunity. They merely result from the above-mentioned suboptimal immune responses that are driving immune escape of the virus, which is now primarily transmitted through asymptomatic to mild infections via (unprotected) contacts among C-19 vaccinees.
So, please, guys, wake up and be prepared! Seriously!!
“Ministers have repeatedly said they won’t resort to imposing lockdowns unless a doomsday variant” (https://www.dailymail.co.uk/health/article-13416469/Health-chiefs-issue-alert-new-Covid-variant-FLiRT-sweeping-UK.html). Unfortunately, that doomsday variant is now well on its way to staging a ‘coup.’
In the absence of any rational plan (which, of course, must not include vaccination!), its emergence will inevitably cause the health care system to collapse. This, together with the societal chaos such a collapse will generate, will leave officials with no other solution than to impose draconian lockdowns.
Believe me, I do not relish sharing these viewpoints, but I can tell you with all transparency and honesty that I am telling you the truth and nothing but the truth.
‘When you have eliminated all which is impossible, then whatever remains, however improbable, must be the truth’
(Arthur Conan Doyle, The Case-Book of Sherlock Holmes)
Recommended for you