Older age is a significant risk factor for serious illness and death for COVID-19, particularly when combined with significant underlying health conditions.
Today’s data shows that 100% of the deaths today were people over 60; averaging out to 98% for the last 7 days or 90.9% for people over 70 (79% of deaths were among the jabbed in the last 7 days).
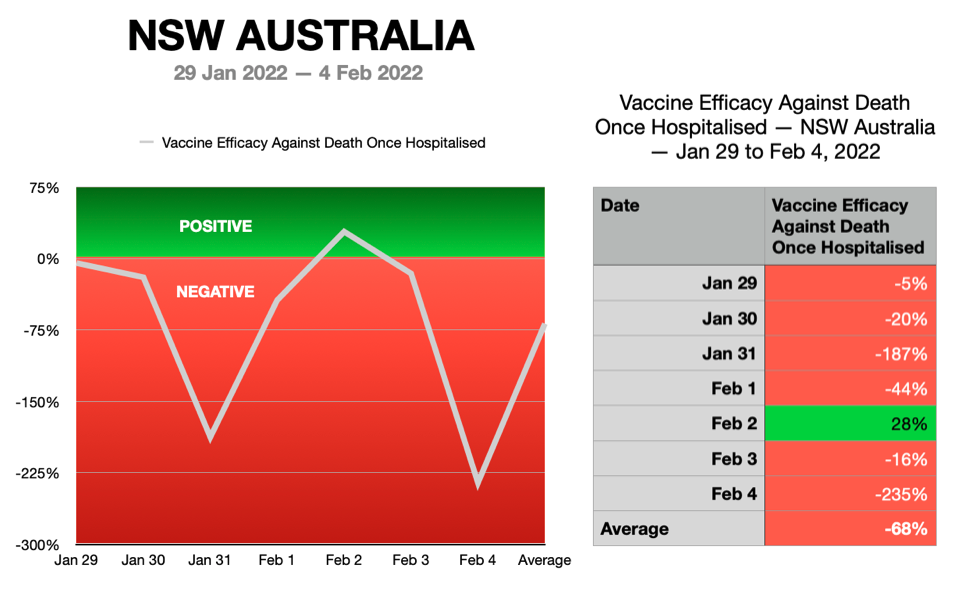
Vaccine Efficacy Against Death Once Hospitalised
Vaccine Efficacy Against Death Once Hospitalised for the 4th of February, 2022 was calculated to be NEGATIVE at -235%.
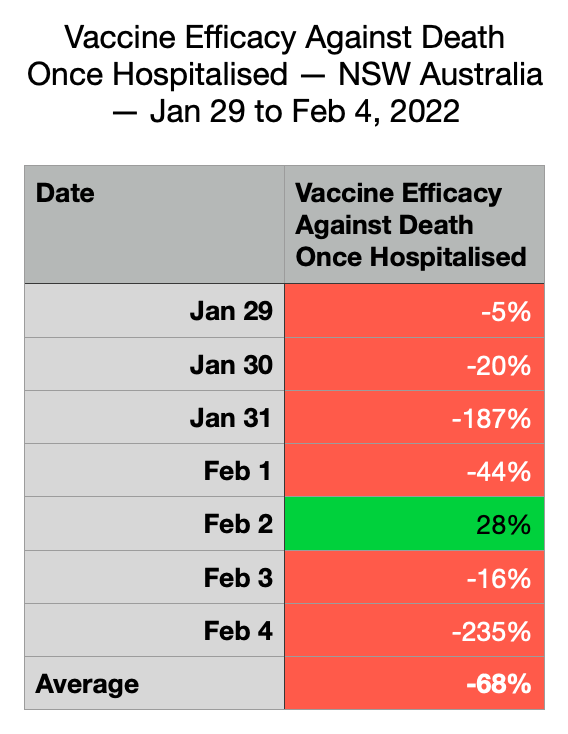
The 7 day moving average was calculated to be NEGATIVE at -68% (254 lives lost).
Hospitalised vs Mortality With Vaccine Status
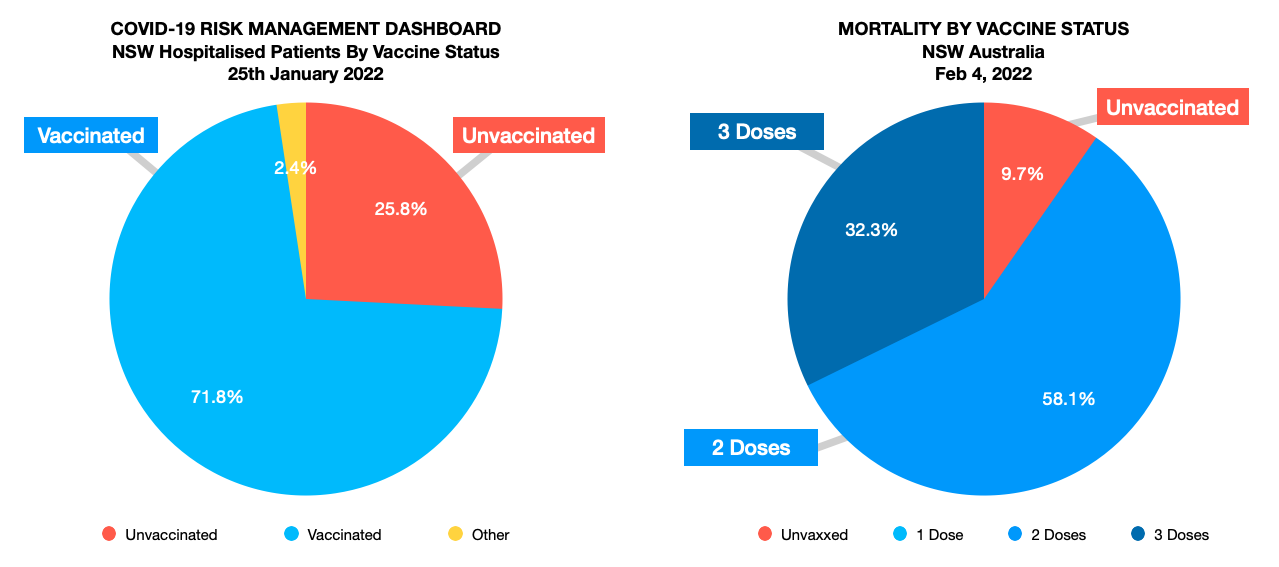
For hospitalised patients we are not given dose numbers and we are not given an age or comorbidity breakdown. There is also a small number of people with an unknown status classified as ‘other’.
About
Vaccine effectiveness against death once hospitalised simply looks at the latest known hospital occupancy of the vaxxed verses the unvaxxed and the deaths associated with the same cohort.
This calculation is measuring severe cases (hospitalised patients) and then comparing them against the final outcome and the number of deaths for this cohort. Vaccination rate of the population is irrelevant for this calculation as this method does NOT allow the vaccine to receive glory for vaxxing the healthy. This formula is a better measuring stick as it shows the true vaccine efficacy (protection) of the vulnerable who often have comorbidities once hospitalised.
Disclaimer:
We know that COVID-19 disproportionately targets the elderly and sadly the publicly available data provided by NSW Health is incomplete and we do not know the age breakdown or comorbidity of the people in hospital hence our limitations to draw authoritative conclusions. It is simply a snapshot or possible signal showing how the vaccinated compare with the unvaccinated in severe cases (once hospitalised). Therefore the vaccine efficacy once hospitalised against death as calculated here should be treated as a rough guide and should only be applied to the older vulnerable age groups (+50) as they are the ones that are dying and that this data is representing. I will attempt to access all the required data but at this stage these —real world— numbers are what we have to work with.
Please note that we are measuring vaccine efficacy once hospitalised so we are not including vaccination rates in the population but I do give this calculation at the bottom of this blog at the conclusion.
The NSW Health data used shows vaccines reduce hospitalisation (+VE). But why is the majority of the vaccinated patients in hospital doing worse than the minority of the unvaccinated patients relative to their occupancy ratio in hospital. Does the vaccine stop working in hospital?
From many data sources we know the vaccines do not stop infection but they somehow reduce hospitalisation — only to reverse in hospital with a negative efficacy for mortality once hospitalised. This needs explaining else it’s a red flag on the data. The vaccinated should not being doing worse in hospital but they are and by a significant margin.
This calculation could be better if we had hospitalisation data by age group and comorbidity for each individual case and if people are in hospital for COVID-19 or with COVID-19.
Data:
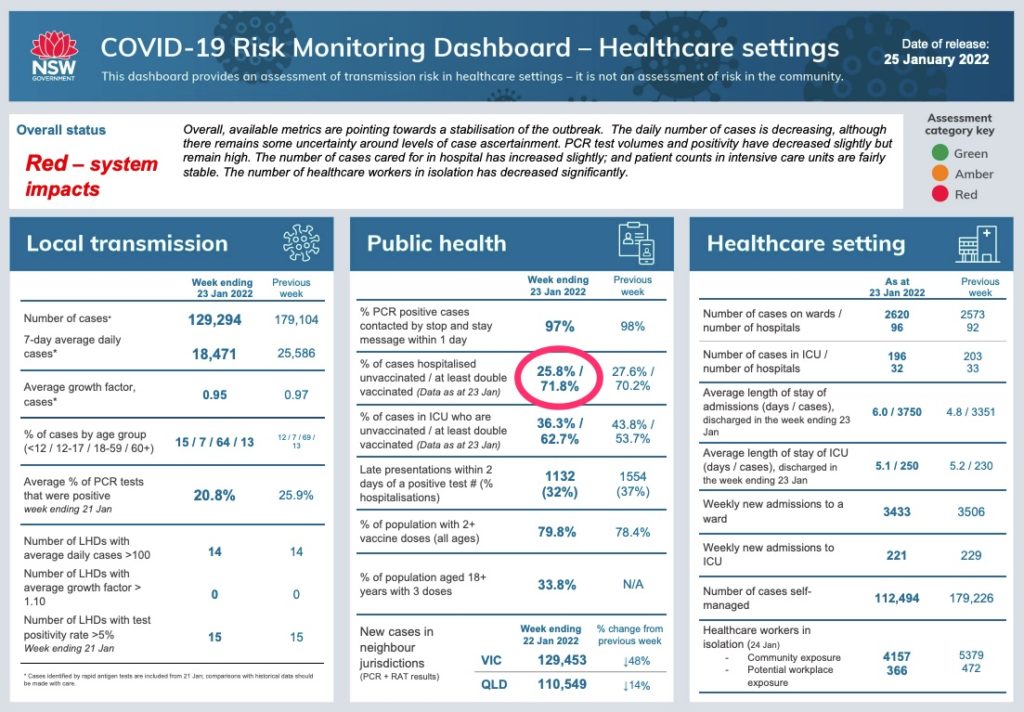
Patients in hospital:
Vaxxed 71.8%
Unvaxxed 25.8%
Other 2.4%
*Data taken from the COVID-19 Risk Management Dashboard put out by NSW Health on the 19th of January. This data is not broken down by dose, age or comorbidity. I am attempting to find better data. For source please see screenshot at the bottom of page with link to the original NSW Health document.
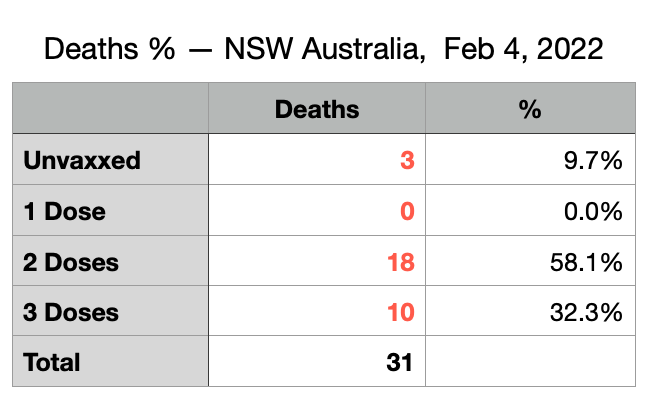
Deaths:
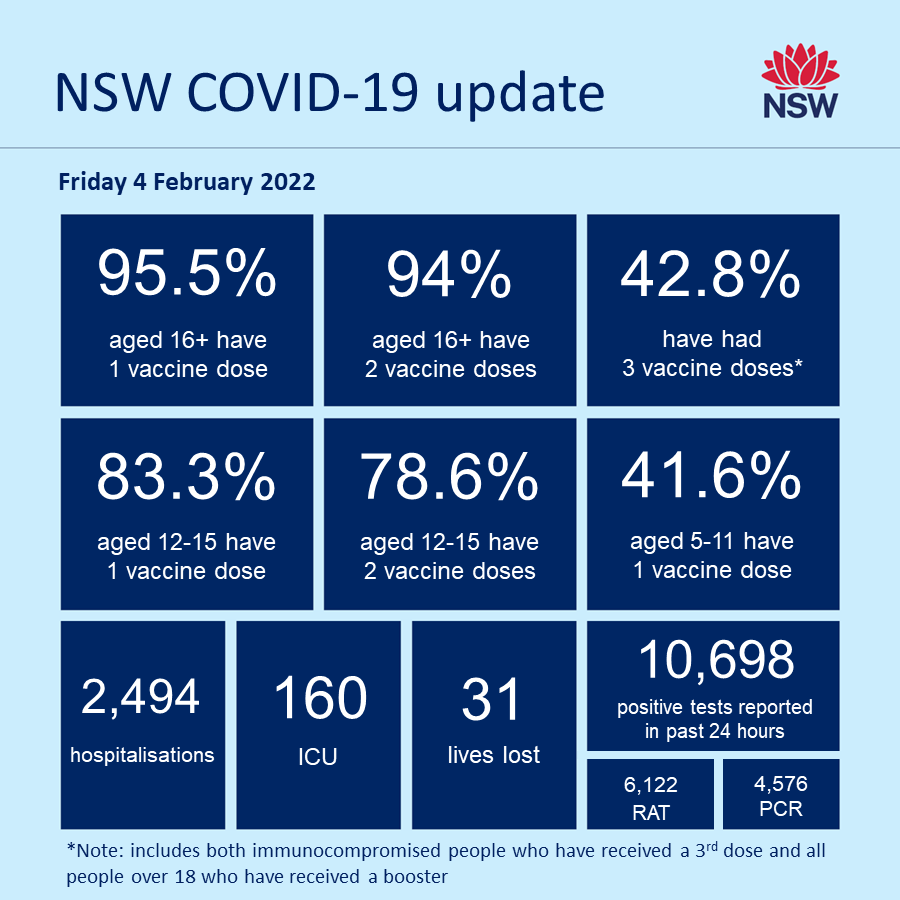
Sadly, NSW Health is today reporting the deaths of 31 people with COVID-19; 21 men and 10 women.
Of the 31 people who died, one person was in their 60s, seven people were in their 70s, 12 people were in their 80s, 10 people were in their 90s, and one person was aged 100.
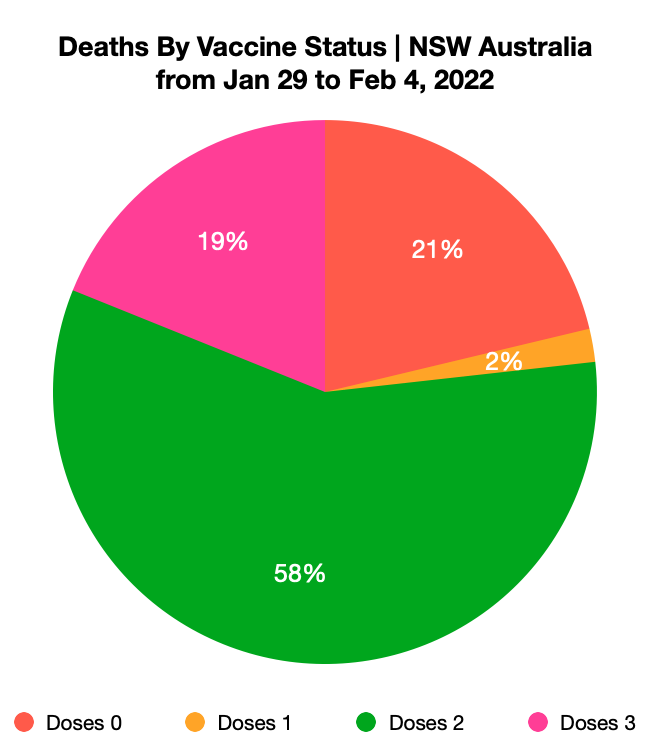
Ten people who died had received three doses of a COVID-19 vaccine, 18 people had received two doses, and three people were not vaccinated.
Triple Vaxxed 10 ppl (32.3%)
Double Vaxxed 18 ppl (58.1%)
Partially Vaxxed 0 ppl (0.0%)
Unvaxxed 3 ppl (9.7%)
*Data taken from NSW Health twitter update with links to the tweets further down this page. Partially vaccinated have been added to the vaccinated because they were either injured by the vaccine and could not take the second shot or it is a direct result of vaccinating during a pandemic which has its own risks for the first 10 days after each shot and is part of the risks attributed to mass vaccination of the whole population.
Calculation:
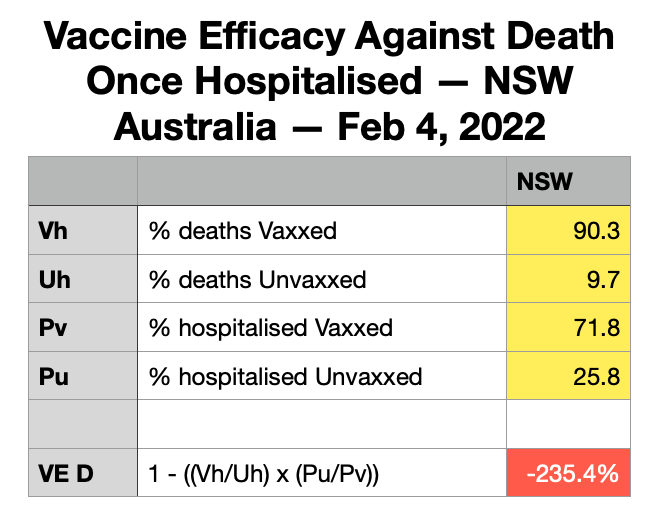
*Above data table shows the calculation to obtain Vaccine Efficacy Against Death Once Hospitalised.
Vaccine Efficacy Against Death Once Hospitalised for February 4, 2022:
= NEGATIVE -235.4%.
Seven Day Average:
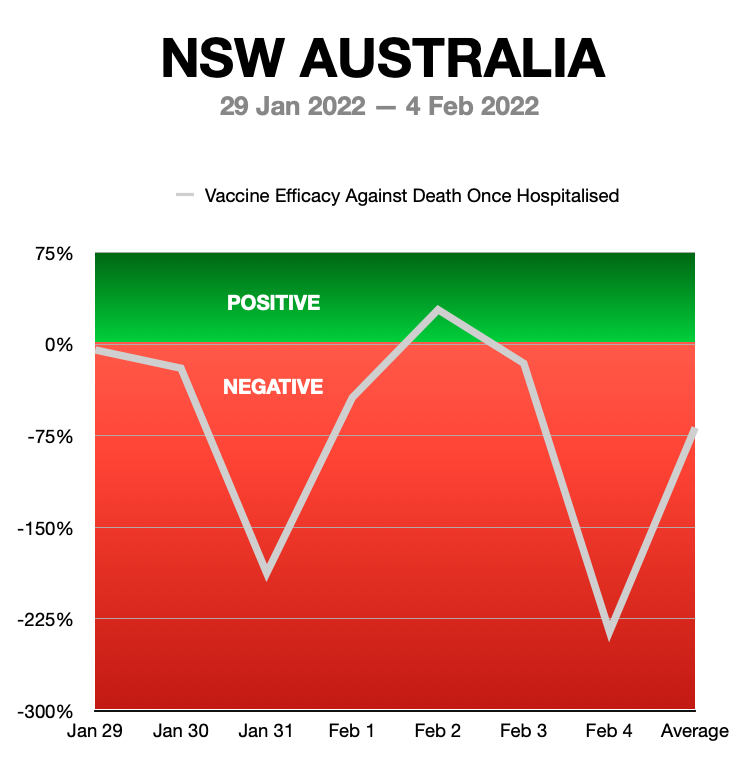
The 7 Day Moving Average Vaccine Efficacy Against Death Once Hospitalised for the period starting from January 29, 2022 to February 4, 2022
= NEGATIVE -68%
Deaths by Dose, Comorbidity And Age Breakdown
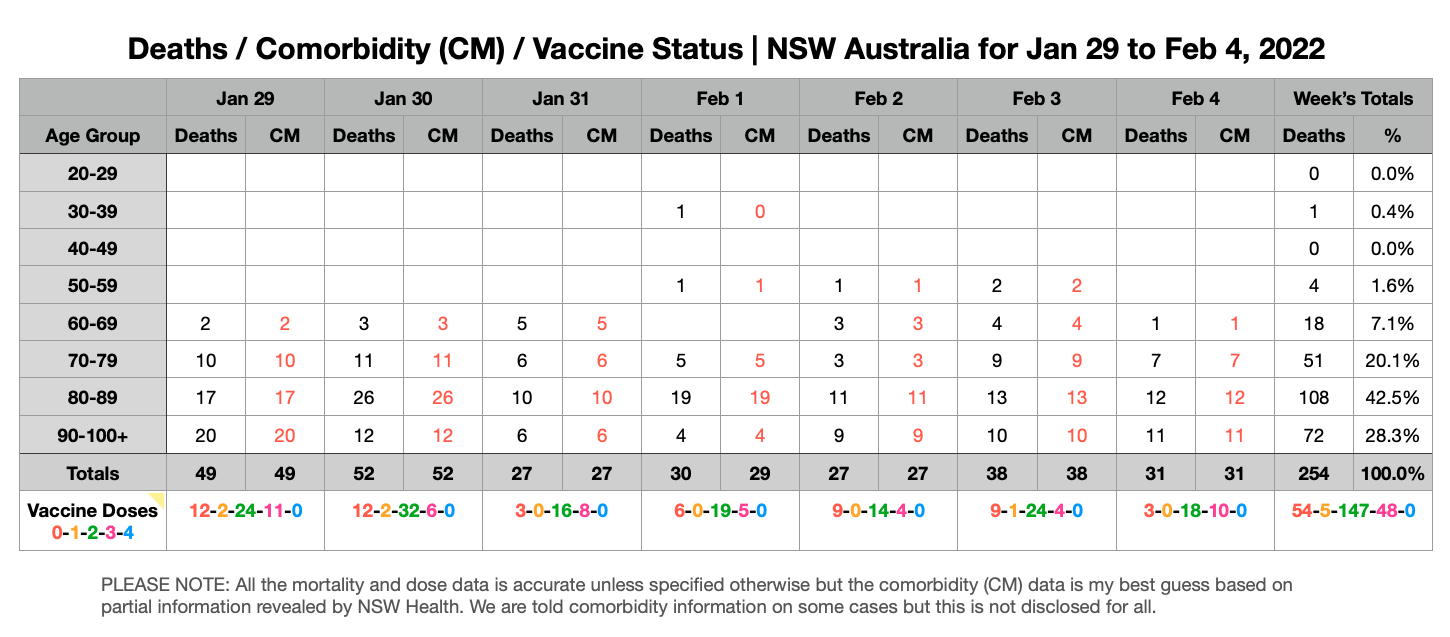

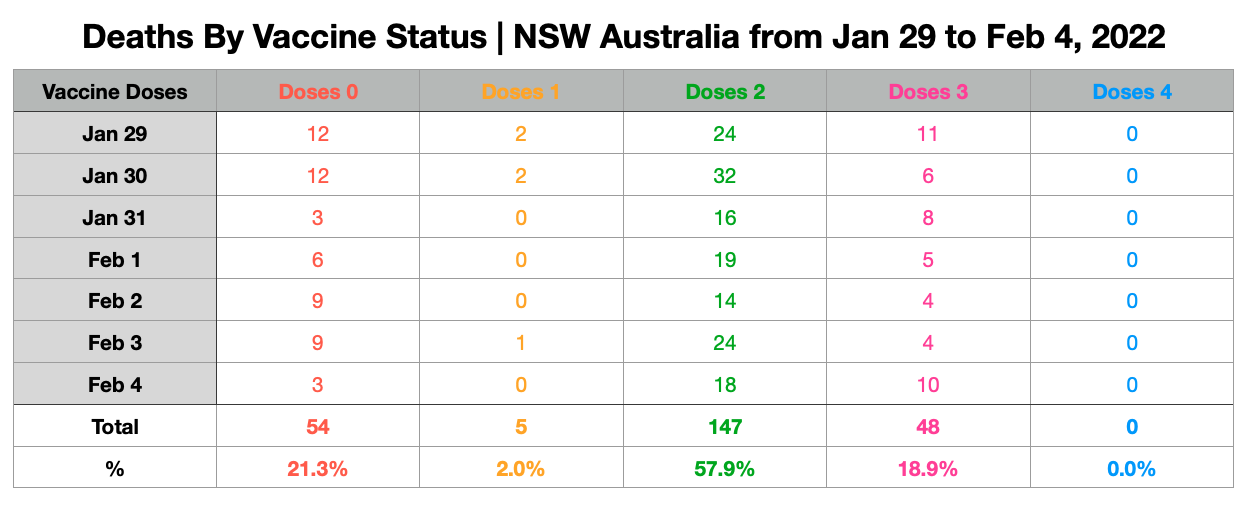
*We do not get a detailed list of vaccine status for each case and age group but we do get totals per age group and sometimes they give us the comorbidity details as well.
Today’s Conclusion
If we accept that 94% of the adults in NSW over 50 are vaccinated; vaccine efficacy against death by considering the relative vaccination rates would only be a POSITIVE 40%.
Therefore it is clear that blocking early treatment with such low vaccine efficacy is a crime against the Australian people.
Both the vaccinated and unvaccinated require early treatment especially if the individual is elderly with multiple comorbidities.
There should be no reason for negative vaccine efficacy when a vaccinated person is hospitalised. Why is this stage so bad for the vaccinated? This is worthy of further study and an explanation.
Data Source:
Hospital Occupancy Data By Vaccine Status Was taken From The COVID-19 Risk Management Dashboard
https://aci.health.nsw.gov.au/
NOTE:
Please remember I currently do not have access to detail mortality data broken down by age and vaccine status so the signal reliability will be crude and perhaps should only be applied to get an indication how well the vaccine protect the vulnerable (elderly).
Recommended for you